
Walk into any pharmacy, grocery store, or scroll through social media long enough, and you’ll be confronted by an overwhelming wall of vitamins, minerals, and supplements — each promising to boost your energy, strengthen your immunity, improve your skin, or protect your heart. The global supplement industry is now worth over $150 billion annually, and more than half of all U.S. adults report taking at least one dietary supplement each month.
But here’s what I want you to know as your physician: the marketing has far outpaced the evidence.
That doesn’t mean supplements are useless — some are genuinely important for specific people in specific circumstances. But it does mean that before you spend money on something you’re swallowing every day, you deserve a clear, honest look at what the science actually says. This post is that look.
What Vitamins and Minerals Actually Are
Vitamins and minerals are micronutrients — compounds the body requires in small amounts to carry out essential metabolic functions. The key word is essential: your body cannot manufacture most of them on its own, so they must come from food.
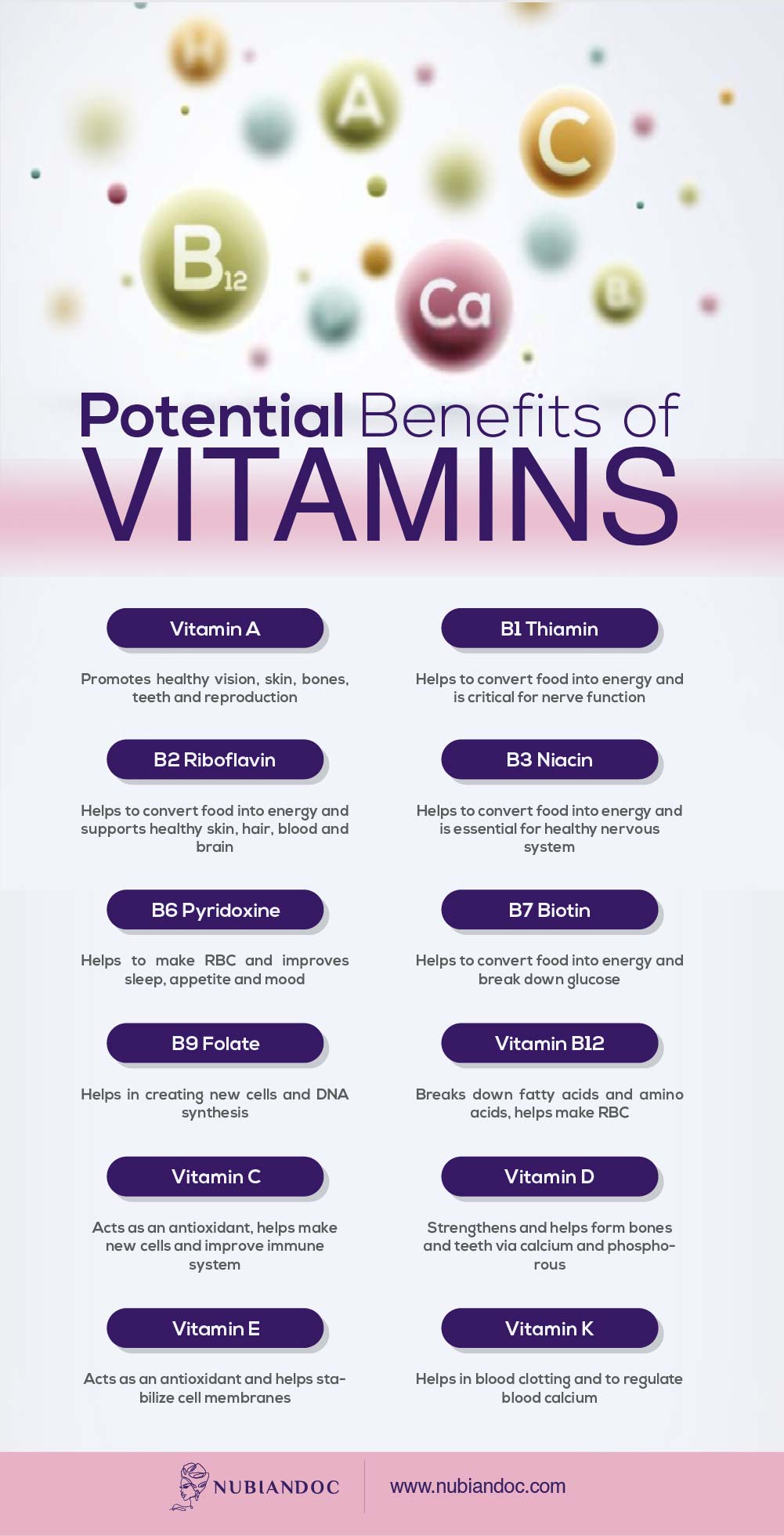
Vitamins are organic compounds found in plants and animals. They fall into two categories:
- Fat-soluble vitamins (A, D, E, K) are absorbed alongside dietary fats and stored in the liver and fatty tissue. Because they accumulate in the body, they carry a higher risk of toxicity if over-supplemented.
- Water-soluble vitamins (C and the B-complex family — B6, B12, folate, niacin, riboflavin, thiamin, biotin) dissolve in water, are not stored in significant quantities, and excess amounts are filtered out by the kidneys. They need to be replenished more regularly through food.
Minerals are inorganic elements — calcium, iron, magnesium, zinc, iodine, potassium, and others — that support bone structure, nerve function, fluid balance, and hundreds of enzymatic processes throughout the body.
The best — and most bioavailable — source of all of these is a varied, whole-food diet. Supplements are not a replacement for food. They are, at best, a targeted tool for specific gaps.
What the Medical Evidence Actually Says About Supplements
This is the part most supplement marketing glosses over entirely.
In 2022, the U.S. Preventive Services Task Force (USPSTF) — the independent expert body that evaluates preventive health evidence — issued its updated recommendations on vitamin and mineral supplementation for healthy, non-pregnant adults. After reviewing 84 studies, including large, well-designed randomized controlled trials, their conclusions were sobering:
- Beta carotene and vitamin E supplements for preventing cardiovascular disease or cancer: DO NOT USE. The USPSTF issued a formal “D” recommendation — meaning the harms outweigh the benefits. Beta carotene has been shown to increase the risk of lung cancer, particularly in smokers.
- Multivitamins for preventing cardiovascular disease or cancer: INSUFFICIENT EVIDENCE. The task force could neither recommend for nor against them — because the current evidence simply doesn’t support using them for these purposes.
- Most individual supplements for preventing cardiovascular disease or cancer: INSUFFICIENT EVIDENCE.
Additionally, in December 2024, the USPSTF issued a draft recommendation against vitamin D supplementation for the purpose of preventing falls or fractures in postmenopausal women and older men — reversing earlier guidance that had supported it.
The takeaway is not that supplements are dangerous across the board. It’s that for healthy adults without known deficiencies, taking supplements to prevent chronic disease is largely an unsupported investment. The evidence simply isn’t there.
What IS supported by evidence is supplementing to correct a diagnosed or clinically suspected deficiency — and for certain populations, that is both appropriate and important. More on that below.
Important Caveat: The FDA Does Not Approve Supplements
Before we go further, this matters: unlike prescription medications, the FDA does not review dietary supplements for safety or effectiveness before they reach the market. Manufacturers are not required to prove a supplement works — only to submit safety data if the product contains a new ingredient. The FDA categorizes supplements as food, not drugs.
This means:
- There is no standardized list of ingredients across brands
- Dosing can vary widely between products
- Label claims are not independently verified
- Quality control varies enormously by manufacturer
If you do choose to supplement, look for products that carry third-party verification seals — NSF International, USP (U.S. Pharmacopeia), or ConsumerLab — which indicate the product has been independently tested for purity and potency.
Supplements With Genuine, Evidence-Based Relevance for Women
Here is where I want to be specific, because this is where individual context — your health history, your lab values, your life stage — matters enormously.
Vitamin D
Vitamin D is arguably the most clinically significant deficiency I see in practice, and it is disproportionately common in women with darker skin tones. Melanin reduces the skin’s ability to synthesize vitamin D from sunlight — meaning that regardless of where you live, darker skin requires significantly more sun exposure to produce the same amount of vitamin D as lighter skin.
A 2025 NHANES-based analysis found that only 17.3% of non-Hispanic Black women met vitamin D sufficiency criteria. Research consistently links low vitamin D status to increased risk of adverse pregnancy outcomes, bone disease, immune dysfunction, and metabolic conditions. If you haven’t had your 25-hydroxyvitamin D level checked recently, ask your physician to include it in your next blood panel.
Sufficiency is generally defined as a serum level ≥30 ng/mL. Supplementing with vitamin D₃ (the most bioavailable form) is appropriate when lab-confirmed deficiency or insufficiency is present. Dose and duration should be guided by your provider based on your levels — not by what’s on the shelf.
Iron
Iron deficiency is the most common nutritional deficiency worldwide and disproportionately affects women of reproductive age due to menstrual blood loss. Symptoms — fatigue, brain fog, shortness of breath, poor exercise tolerance, hair shedding — are often dismissed or attributed to other causes. Non-anemic iron deficiency (low ferritin without frank anemia) can cause all of these symptoms before a CBC shows any abnormality.
Ask your provider to check both a CBC and a serum ferritin — ferritin below 30 μg/L is consistent with iron deficiency even with a normal hemoglobin. If you are experiencing heavy periods, are vegetarian or vegan, or are pregnant, iron status should be on your radar.
Iron supplements should only be taken when deficiency is confirmed — excess iron carries its own health risks and can interfere with absorption of other minerals.
Folate (Folic Acid)
This is one of the most clearly evidence-supported supplement recommendations in all of medicine. The USPSTF recommends that all individuals who are pregnant or capable of becoming pregnant take 0.4–0.8 mg (400–800 mcg) of folic acid daily to prevent neural tube defects. Because neural tube development begins within the first few weeks of pregnancy — often before a woman knows she is pregnant — this supplementation should begin before conception, not after a positive test.
Food sources include leafy greens, legumes, fortified grains, and citrus — but supplementation is the standard of care for reproductive-age women regardless of diet quality.
Magnesium
Magnesium is involved in over 300 enzymatic reactions in the body — including blood sugar regulation, nerve function, heart rhythm, blood pressure, muscle contraction, and sleep. Despite this, most Americans fall short of the recommended daily intake.
For women specifically, emerging evidence is particularly interesting. A 2025 narrative review found that women with PMS have lower magnesium levels than those without, and multiple clinical trials have demonstrated that magnesium supplementation significantly improves emotional and physical PMS symptoms — including irritability, depression, fatigue, and anxiety. Estrogen fluctuations across the menstrual cycle, pregnancy, and menopause affect magnesium absorption and retention, making women’s magnesium needs particularly dynamic.
Magnesium also supports bone health, helps regulate blood pressure, and is associated with reduced migraine frequency. Magnesium glycinate and magnesium citrate tend to be better tolerated than magnesium oxide, which is poorly absorbed.
Note: If you have kidney disease, heart disease, or diabetes, check with your provider before starting magnesium — it can interact with certain medications.
Vitamin B12
B12 deficiency is most commonly seen in people following vegan or strict vegetarian diets (B12 is found almost exclusively in animal products), adults over 50 (stomach acid production declines with age, reducing B12 absorption), individuals taking metformin for diabetes or long-term proton pump inhibitors (PPIs), and people who have undergone gastric bypass surgery. Deficiency leads to fatigue, neurological symptoms, and a form of anemia. If you fall into any of these categories, B12 status should be monitored and supplemented as needed.
Prenatal Vitamins
For pregnant individuals or those actively trying to conceive, a quality prenatal vitamin is not optional — it is standard care. Look for one that includes folate (or folic acid), iron, iodine, DHA, choline, calcium, and vitamin D. Not all prenatal vitamins are equal; some contain methylfolate (the activated form), which is better utilized by people with MTHFR gene variants.
Who May Benefit From a Multivitamin
Despite the limited evidence for multivitamins in healthy adults, there are populations for whom they are clinically reasonable:
- People with restrictive eating or very low caloric intake (under 1,200 calories/day)
- Those with malabsorption conditions — Crohn’s disease, celiac disease, ulcerative colitis, IBS
- Post-bariatric surgery patients, who have significantly altered nutrient absorption
- Older adults with reduced appetite, food variety, or absorption
- Those with chronic illness that compromises nutritional status
- People experiencing food insecurity who may have limited dietary variety
- Vegans and vegetarians, who may need B12, iron, zinc, iodine, and omega-3s in addition to a general multivitamin
If you don’t fall into these categories and eat a reasonably varied diet, a multivitamin is unlikely to provide meaningful additional benefit — and for most people, it’s not needed.
When to Take Your Supplements: Timing Matters
How and when you take supplements affects how well your body absorbs them.
Take with food:
- Fat-soluble vitamins (A, D, E, K) must be taken with a meal containing fat to be absorbed properly
- Iron is better absorbed with vitamin C (e.g., a glass of orange juice), but should not be taken with calcium — they compete for absorption
- Magnesium is generally better tolerated with food
Timing recommendations:
- Morning: Vitamin D, vitamin C, B-complex vitamins (they can be energizing)
- Evening: Magnesium (supports sleep and muscle relaxation), vitamin B3 (niacin)
- Avoid combining: Calcium and iron, zinc and copper, fat-soluble vitamins without food
The Cleveland Clinic has a helpful, practical breakdown of supplement timing if you want a reference to bookmark.

The Toxicity Risk: More Is Not Better
Overconsumption of certain vitamins — particularly fat-soluble ones — can be harmful. Hypervitaminosis (vitamin toxicity) most commonly occurs with vitamins A, D, E, and K, since these are stored in the body rather than excreted. Symptoms of vitamin A toxicity include nausea, liver damage, and in severe cases, increased intracranial pressure. Excessive vitamin D can cause dangerous elevations in blood calcium. The American Association of Poison Control Centers has documented tens of thousands of annual exposures to vitamin overdose, with the majority involving young children.
More is not better. Supplements should be dosed based on need, not on a general more-is-more logic.
A Word on the Supplement Industry’s Marketing
I want to be direct about something. The supplement industry is built on a fundamental asymmetry: the burden of proof for supplements is far lower than for medications, and the marketing is designed to close that gap through implication rather than evidence. Words like “supports,” “promotes,” and “may help” are not the same as “proven to treat” or “clinically shown to prevent.” They are legal hedges.
When a product claims to “support immune health” or “promote energy,” it is not making a medical claim — and it isn’t required to prove anything. The result is that billions of dollars are spent annually on supplements with minimal to no evidence of benefit for the people taking them.
That said, I am not anti-supplement. I prescribe and recommend them regularly — when there is a clinical reason, based on individual assessment and lab data. The difference is targeted supplementation based on evidence versus general supplementation based on marketing.
Know the difference. Your health — and your wallet — will benefit.
The Bottom Line
Here is what the evidence supports as of 2025:
- For healthy adults without deficiencies: A well-balanced diet remains the best source of vitamins and minerals. Most people do not need a daily multivitamin, and there is insufficient evidence to support taking one to prevent heart disease or cancer.
- Avoid: Beta carotene and vitamin E supplements for chronic disease prevention — the USPSTF recommends against them.
- High-priority for many women: Vitamin D (especially with darker skin or limited sun exposure), iron (especially with heavy periods or plant-based diet), folate (especially if pregnant or planning to be), magnesium (especially with PMS, poor sleep, or high stress).
- Lab-first approach: Before starting any supplement, ask your physician to check relevant levels. Supplementing blindly is both costly and potentially harmful.
- Quality matters: Choose third-party tested products (NSF, USP, ConsumerLab) and be skeptical of products with proprietary blends, excessive claims, or no transparency about sourcing.
If you’re unsure where to start, the best first step is a conversation with your physician and a comprehensive metabolic panel that includes vitamin D, ferritin, B12, and magnesium. Let your labs guide what your body actually needs.
Want to learn more about how nutrition affects your body? Read our posts on intermittent fasting and what the evidence actually says, how added sugar affects your health, and how to maintain a healthy weight.
References:
- USPSTF. Vitamin, Mineral, and Multivitamin Supplementation to Prevent CVD and Cancer. JAMA. 2022.
- USPSTF. Draft Recommendation: Vitamin D, Calcium for Falls and Fractures Prevention. December 2024.
- USPSTF. Folic Acid Supplementation to Prevent Neural Tube Defects.
- Aguilar M et al. Vitamin D Status in Non-Hispanic Black Women: NHANES 2011–2018. J Racial Ethnic Health Disparities. 2025.
- Grant WB et al. Does High Prevalence of Vitamin D Deficiency in African Americans Contribute to Health Disparities? Nutrients. 2021.
- Conforto et al. Magnesium: Exploring Gender Differences in Health Impact. Nutrients. 2025.
- NIH Office of Dietary Supplements. Magnesium Health Professional Fact Sheet.
- Prentice et al. Diagnosis and Management of Iron Deficiency in Females. CMAJ. 2024.
- FDA. Dietary Supplements Overview.