
Pregnancy is one of the most physically demanding experiences a human body can undergo. It is also one of the most medically consequential windows of a woman’s life — a period during which the decisions made, the care received, and the support systems available have lasting implications not just for the nine months of gestation, but for years afterward.
And yet, for far too many women in this country — particularly Black women — that window has not been met with the care it deserves.
Let me be direct about something before we get into the clinical guidance: the United States has one of the highest maternal mortality rates among wealthy nations. In 2024, the CDC reported the overall maternal mortality rate at 17.9 deaths per 100,000 live births. For Black women, that rate was 44.8 per 100,000 — more than three times the rate for white women (14.2) and the only group that did not show a statistically significant decline. This is not a footnote. It is the context within which every recommendation in this post lives.
Knowing what to expect, what is normal, what warrants urgent attention, and how to advocate for yourself within a system that has historically underserved you is not just empowering — it is potentially lifesaving.
This is the guide I wish every patient came in already having read.
Prenatal Care: What’s Changed and What It Means for You
In April 2025, the American College of Obstetricians and Gynecologists (ACOG) released landmark new guidance recommending a fundamental transformation of prenatal care delivery in the United States. The current prenatal care model — fixed visits every 4 weeks until the 7th month, every 2 weeks until the 8th month, then weekly — was developed in 1930 and has changed little since. ACOG’s new guidance, built around the PATH framework (Plan for Appropriate Tailored Healthcare in Pregnancy), calls for:
- A comprehensive needs assessment before 10 weeks of gestation — including medical history, reproductive history, and a structured evaluation of social determinants of health: housing, food access, transportation, domestic safety, and mental health
- Tailored visit schedules based on individual risk — for average-risk pregnancies, evidence supports 6–10 well-designed visits with equivalent outcomes to the traditional 12–14, freeing capacity for higher-risk patients who need more intensive support
- Expanded care modalities — telemedicine, group prenatal care, and remote blood pressure monitoring to reduce barriers and meet patients where they are
- Shared decision-making as the standard — not a courtesy, but a clinical expectation
This matters especially for women navigating work, caregiving, transportation challenges, and a healthcare system that has not always been responsive to their concerns. If your provider hasn’t discussed your care plan with you as a conversation rather than a prescription, that is worth raising directly.
The First Trimester: What to Expect and What Gets Checked
Your first prenatal visit — ideally before 10 weeks — is one of the most information-dense appointments of your entire pregnancy. It establishes your baseline, identifies risk factors, and sets the tone for your care.
Standard first trimester screening typically includes:
- Complete blood count (CBC): Checks for anemia (low hemoglobin) and thrombocytopenia (low platelet count, affecting clotting)
- Blood type and Rh factor: If you are Rh-negative and the baby’s father is Rh-positive, your body may develop antibodies against the baby’s blood — preventable with Rhogam administered around 28 weeks
- Immunity screening: Rubella (measles), Varicella (chickenpox), Hepatitis B, Hepatitis C, and HIV
- STI screening: Gonorrhea, Chlamydia, Syphilis — all are treatable and all have direct implications for fetal health if untreated
- Genetic carrier screening: Sickle cell disease, Cystic fibrosis, and others depending on family history and ethnicity
- Gestational diabetes risk assessment: A glucose challenge test is offered to at-risk individuals — women with obesity, PCOS, family history of diabetes, or a prior gestational diabetes pregnancy
- Urinalysis and urine culture: Asymptomatic urinary tract infections are common in pregnancy and can trigger preterm labor if untreated
- Group B Streptococcus (GBS): Typically screened later (35–37 weeks), but worth knowing about — GBS colonization is treated with antibiotics during labor to protect the newborn
- Cell-free DNA screening and nuchal translucency ultrasound for chromosomal conditions such as Down syndrome, Trisomy 18, and Trisomy 13 — typically offered between 10–14 weeks
A note on preeclampsia risk: Black women are approximately 60% more likely to develop preeclampsia and face a five times greater risk of dying from it than white women. If you have risk factors — first pregnancy, obesity, chronic hypertension, diabetes, kidney disease, autoimmune conditions, or a family history of preeclampsia — ask your provider specifically about low-dose aspirin prophylaxis, which ACOG recommends starting between 12–28 weeks for high-risk individuals. Know the warning signs: sudden severe headache, vision changes, severe upper abdominal pain, sudden significant swelling of the hands and face, or decreased fetal movement. These are urgent symptoms that require same-day evaluation.
Healthy Weight Gain During Pregnancy
Weight gain in pregnancy is not optional — it is necessary for fetal growth, amniotic fluid production, placental development, and maternal blood volume expansion. But the amount matters, and “eating for two” is a myth that the evidence does not support.
The Institute of Medicine / National Academies guidelines — used by ACOG — establish the following recommended ranges based on pre-pregnancy BMI:
| Pre-Pregnancy BMI | Category | Recommended Gain |
|---|---|---|
| Below 18.5 | Underweight | 28–40 lbs |
| 18.5–24.9 | Normal weight | 25–35 lbs |
| 25.0–29.9 | Overweight | 15–25 lbs |
| 30.0 and above | Obesity | 11–20 lbs |
For women carrying twins, these ranges are higher — discuss specific targets with your provider.
Weight gain should be gradual and distributed across trimesters. In the first trimester, minimal gain (0–2 lbs for average-weight women) is typical as nausea often reduces appetite. In the second and third trimesters, gaining approximately 1 lb per week is generally appropriate for normal-weight women.
Too little weight gain is associated with preterm birth and low birth weight. Excess weight gain is linked to gestational diabetes, gestational hypertension, large-for-gestational-age infants (which increases cesarean risk), and higher postpartum weight retention. Neither extreme is neutral.
If you started pregnancy above a healthy BMI range, this is not a time for intentional weight loss — it is a time for quality nutrition with appropriate caloric support. Work with your provider on a realistic, individualized target.
Nutrition During Pregnancy: What Actually Matters
A healthy pregnancy diet is not complicated — but it is specific. Here is what the evidence emphasizes.
Start With Folate — Before You’re Pregnant
Folate (folic acid) is the single most critical preconception nutrient. The neural tube — which becomes the baby’s brain and spinal cord — closes between days 17 and 30 after conception, often before a woman even knows she is pregnant. Neural tube defects, including spina bifida and anencephaly, are significantly reduced by adequate folate intake.
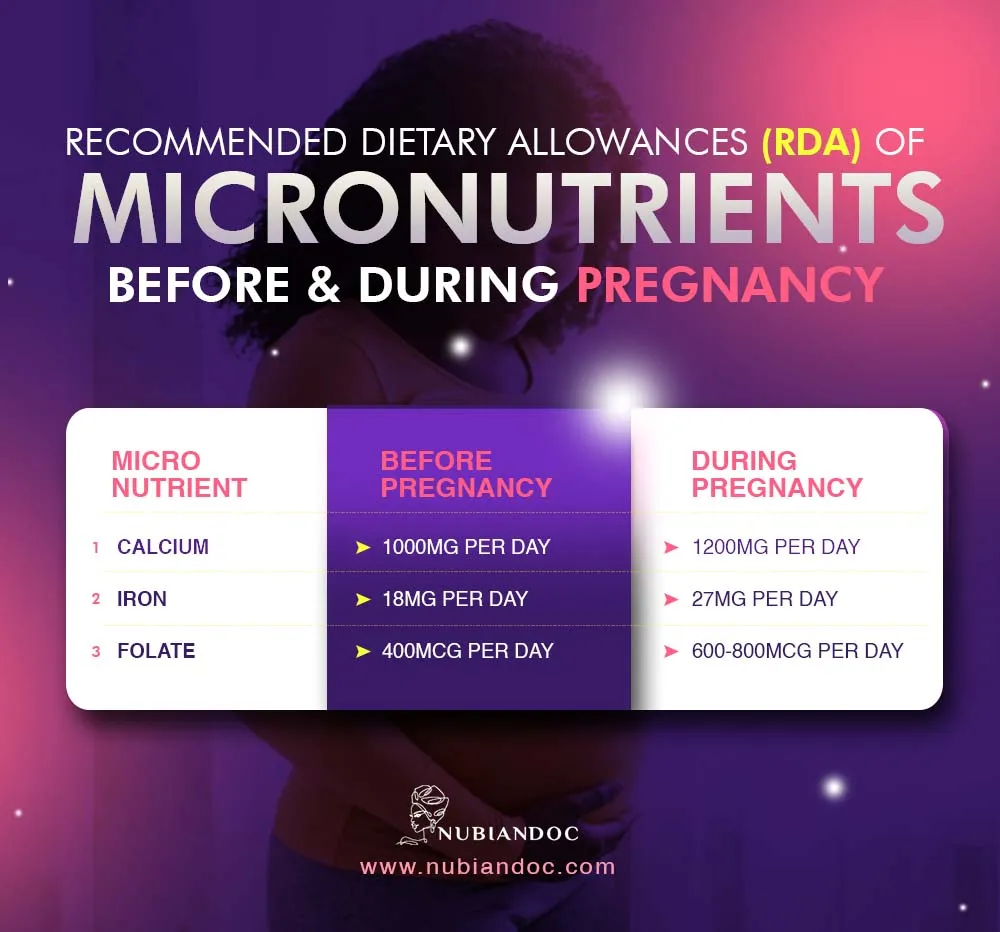
ACOG recommends 400–800 mcg of folic acid daily, beginning at least one month before conception and continuing through the first trimester. Food sources include leafy greens (spinach, kale, collard greens), lentils, beans, avocado, and fortified cereals — but supplementation through a prenatal vitamin is the standard of care because food sources alone are rarely sufficient.
Iron: The Most Common Deficiency in Pregnancy
Pregnancy increases your blood volume by up to 50% — and iron is what makes that possible. The recommended intake during pregnancy is 27 mg per day, compared to 18 mg for non-pregnant women. Iron deficiency anemia in pregnancy is associated with preterm birth, low birth weight, and maternal fatigue severe enough to affect daily function.
Iron-rich foods include lean red meat, poultry, fish, eggs, lentils, beans, tofu, and dark leafy greens. Pairing iron-rich foods with vitamin C (citrus, strawberries, bell peppers) significantly improves absorption. Avoid taking iron with calcium supplements or dairy — they compete for absorption. If your provider diagnoses iron deficiency, supplemental iron beyond your prenatal vitamin will be recommended. See our post on vitamin supplementation and iron testing for more on how ferritin and CBC work together.
DHA and Omega-3 Fatty Acids
DHA (docosahexaenoic acid) is an omega-3 fatty acid essential for fetal brain and eye development, particularly in the third trimester when brain growth accelerates rapidly. The best dietary sources are fatty fish — salmon, sardines, herring, and trout. Most prenatal vitamins contain DHA; confirm yours does.
A note on fish safety during pregnancy: Fish is nutritious and recommended, but mercury content matters. The FDA advises eating 2–3 servings per week of low-mercury fish (salmon, canned light tuna, tilapia, shrimp, catfish) and avoiding high-mercury fish entirely (shark, swordfish, king mackerel, tilefish, bigeye tuna).
Calcium and Vitamin D
Calcium supports fetal bone and tooth development. If your intake is inadequate, the baby will draw calcium from your bones. Aim for 1,000 mg daily through low-fat dairy, fortified plant milks, leafy greens, almonds, and sardines with bones.
Vitamin D works with calcium for bone health and immune function — and, as we cover in detail in our post on vitamin supplementation, deficiency is significantly more common in women with darker skin tones due to melanin’s effect on cutaneous vitamin D synthesis. Ask your provider to check your 25-OH vitamin D level if it hasn’t been done recently.
Build Your Plate Around Whole Foods
The foundation of a healthy pregnancy diet is the same as a healthy diet at any time — just with higher nutritional stakes:
- Vegetables and fruits at every meal — aim for color variety for the broadest micronutrient coverage
- Whole grains (brown rice, oats, whole wheat, quinoa) for sustained energy, B vitamins, and fiber
- Lean protein at each meal — eggs, legumes, poultry, fish, Greek yogurt, cottage cheese
- Healthy fats — avocado, nuts, seeds, olive oil, fatty fish
- Adequate fiber to manage the constipation that affects most pregnant women, especially in the third trimester
What to Limit and Avoid
| Substance | Recommendation | Why |
|---|---|---|
| Alcohol | Avoid entirely | No safe amount has been established; linked to fetal alcohol spectrum disorders, miscarriage, stillbirth |
| Caffeine | Limit to under 200 mg/day (~1 small coffee) | Higher intake associated with increased miscarriage risk and low birth weight |
| Raw or undercooked meat, fish, eggs | Avoid | Risk of Listeria, Salmonella, Toxoplasma — all dangerous to the fetus |
| High-mercury fish | Avoid | Neurotoxic to the developing fetal brain |
| Unpasteurized dairy and juice | Avoid | Risk of Listeria and E. coli |
| Smoking | Avoid entirely | Associated with placental abruption, placenta previa, preterm birth, low birth weight, SIDS |
| Recreational drugs | Avoid entirely | No safe exposure level established for any substance |
On smoking: If you smoke and are pregnant or planning to be, this is a clinical priority. Resources including 1-800-QUIT-NOW and behavioral counseling are available. Your provider can help without judgment.
Hydration During Pregnancy
Fluid needs increase significantly during pregnancy. Your body uses water to form amniotic fluid, expand blood volume, support fetal circulation, deliver nutrients, and — later in pregnancy — reduce constipation and prevent urinary tract infections.
The National Academies of Sciences recommend approximately 10 cups (2.4 liters) of fluid daily during pregnancy from all sources, including water-rich foods. Adequate hydration also supports skin elasticity and may reduce swelling (edema) in the legs and feet.
Signs of adequate hydration: Pale yellow urine, frequent urination. Dark yellow urine is a reliable signal to drink more.
Adequate hydration may also reduce the risk of preterm contractions — dehydration can trigger uterine irritability. If you notice contractions, drinking a large glass of water and resting for 30 minutes is a reasonable first response before calling your provider.

Exercise During Pregnancy: What Is Safe and Why It Matters
Physical activity in pregnancy is not only safe for most women — it is actively beneficial. ACOG recommends at least 150 minutes per week of moderate-intensity aerobic activity for pregnant individuals without contraindications.
Benefits of exercise during pregnancy include:
- Reduced risk of gestational diabetes (by improving insulin sensitivity)
- Lower rates of gestational hypertension and preeclampsia
- Reduced risk of excessive weight gain
- Improved mood and reduced risk of prenatal and postpartum depression
- Better sleep quality
- Reduced duration of labor and lower cesarean rates in some studies
- Faster postpartum recovery
Safe activities during pregnancy:
Brisk walking, swimming, water aerobics, stationary cycling, prenatal yoga, low-impact aerobics, modified strength training, and elliptical exercise are all appropriate. If you were running or doing high-intensity training before pregnancy, you can often continue with modification — discuss with your provider.
Activities to avoid:
Contact sports (basketball, soccer, hockey), activities with fall risk (downhill skiing, horseback riding, gymnastics), scuba diving, hot yoga or hot tubs (core temperature elevation above 102°F is associated with neural tube defects in the first trimester), and lying flat on your back for extended periods after the first trimester (compresses the vena cava).
Warning signs to stop exercising and call your provider: Vaginal bleeding, dizziness or feeling faint, chest pain, severe shortness of breath, calf pain or swelling, decreased fetal movement, uterine contractions, or fluid leaking from the vagina.
Sleep During Pregnancy
Sleep changes dramatically across pregnancy — and poor sleep has real consequences. First trimester fatigue is driven by rising progesterone. The second trimester often brings relief. The third trimester brings new challenges: frequent urination, fetal movement, heartburn, leg cramps, and difficulty finding a comfortable position.
Sleeping on your left side is recommended in the third trimester — it optimizes blood flow to the uterus and kidneys and reduces pressure on the inferior vena cava (the large vein that carries blood from the lower body back to the heart). A pregnancy pillow supporting the abdomen and between the knees can make this significantly more comfortable.
Insomnia and poor sleep in pregnancy are associated with increased rates of gestational diabetes, preeclampsia, preterm birth, and postpartum depression. If you are consistently unable to sleep, this is worth raising at your prenatal visit — it is not just an inconvenience.
Mental Health During and After Pregnancy
Perinatal mental health is one of the most underdiagnosed and undertreated areas of pregnancy care. Anxiety and depression affect approximately 1 in 5 pregnant and postpartum women — and Black women face compounded risk from systemic stressors that are rarely addressed in a standard prenatal visit.
ACOG now recommends screening for anxiety and depression at the initial prenatal visit, again during pregnancy, and at postpartum visits using validated tools. If your provider has not screened you, you can ask for it.
Postpartum depression (PPD) is not the same as the “baby blues.” The baby blues — mild mood fluctuations, tearfulness, and anxiety in the first 1–2 weeks after delivery — are hormonally driven and typically resolve on their own. PPD is a clinical diagnosis characterized by persistent sadness, inability to bond with the baby, hopelessness, difficulty functioning, or intrusive thoughts lasting beyond two weeks postpartum or beginning any time in the first year. It is common, treatable, and not a reflection of your character or your love for your child.
Warning signs that require prompt evaluation:
- Persistent sadness, emptiness, or hopelessness beyond two weeks postpartum
- Difficulty sleeping even when the baby sleeps
- Inability to care for yourself or the baby
- Withdrawing from family and support
- Intrusive or frightening thoughts about harming yourself or the baby
- Feeling disconnected from your baby
If you are experiencing any of these symptoms, contact your provider. The Postpartum Support International helpline (1-800-944-4773) is also available in English and Spanish, 24 hours.
Sleep as a New Mother: Practical Strategies
Sleep deprivation in the newborn period is real and physiologically significant. Chronic sleep loss impairs immune function, impairs judgment, worsens mood, and — particularly relevant postpartum — significantly increases risk of postpartum depression. This is not about willpower. It is biology.
Practical strategies that help:
Divide nighttime duties. If your baby is bottle-fed or you are pumping, a partner can take feeds on alternating nights or handle one full overnight stretch while you sleep uninterrupted. Even one 4–5 hour block of consecutive sleep is significantly more restorative than fragmented sleep across 8 hours.
Sleep when the baby sleeps — selectively, not compulsively. This advice is overused, but in the early weeks, a 60–90 minute nap during the baby’s longest daytime stretch has real physiological benefit.
Limit caffeine timing. Caffeine consumed after 2 p.m. meaningfully disrupts nighttime sleep quality, even if you feel you can fall asleep. If you are breastfeeding, note that caffeine passes into breast milk in trace amounts — keeping intake under 300 mg/day is generally considered safe for most breastfed infants, though some infants are more sensitive.
Protect screens before sleep. Blue light from phones and tablets suppresses melatonin. Setting your phone to night mode and avoiding screens in the 30 minutes before sleep supports your body’s natural sleep onset, however limited the window.
Receive help without guilt. If someone offers to hold the baby while you sleep — say yes. Accepting support is not a concession. It is a clinical strategy.
A Word on Advocating for Yourself in the Healthcare System
This cannot go unsaid.
Research — including a 2025 study published in International Journal for Equity in Health — documents that Black women’s pain and symptoms are more frequently dismissed or undertreated by healthcare providers. The leading causes of pregnancy-related death among Black women — preeclampsia, postpartum cardiomyopathy, hemorrhage — are conditions that respond to timely intervention. When symptoms are ignored or minimized, that window closes.
You have the right to be taken seriously. You have the right to ask questions and receive answers in language you understand. You have the right to a second opinion. If something feels wrong — a sudden severe headache that doesn’t resolve, vision changes, severe upper abdominal pain, a leg that is swollen and painful on one side, decreased fetal movement, chest pain or difficulty breathing — do not wait to be believed. Go to an emergency room.
The CDC’s Hear Her campaign was created specifically to address the pattern of dismissed symptoms in maternal care. It exists because the problem is documented. Knowing this gives you permission to advocate loudly.

Skincare During Pregnancy: What’s Safe, What to Swap, and What to Stop
Your skin changes significantly during pregnancy — and for many women, those changes are among the most noticeable and frustrating parts of the experience. Hormonal surges drive increased sebum production (hello, breakouts), hyperpigmentation (the “mask of pregnancy,” or melasma), stretch marks, dryness, and heightened sensitivity. The question most women have is reasonable: can I still use my regular skincare products?
The answer depends entirely on what’s in them. Some ingredients are well-established as safe. Others carry enough absorption risk or limited safety data that most clinicians — and the American Academy of Dermatology (AAD) — recommend avoiding them during pregnancy. Here is what you need to know.
Ingredients to AVOID During Pregnancy
Retinoids (Vitamin A derivatives) This is the most important category to know. Retinoids — including prescription tretinoin (Retin-A), adapalene (Differin), tazarotene (Tazorac), and over-the-counter retinol — are among the most effective anti-aging and acne ingredients available. They are also the ones dermatologists most consistently recommend stopping during pregnancy. High-dose oral vitamin A is a known teratogen; while topical absorption is lower, four published case reports link topical retinoid use to birth defects consistent with retinoid embryopathy, and the precautionary principle applies. Stop retinoids before conceiving if possible, and do not use them during pregnancy or breastfeeding.
On labels, look for: retinol, retinal, retinoic acid, retinyl palmitate, retinyl linoleate, tretinoin, adapalene, tazarotene.
Hydroquinone Hydroquinone is the most commonly used skin-lightening agent — and one of the most relevant to this audience, given that melasma disproportionately affects women with darker skin tones. The problem is absorption: research estimates 35–45% systemic absorption with topical hydroquinone — significantly higher than most other skincare ingredients. While no increased risk of birth defects has been confirmed, the absorption rate warrants caution, and the AAD recommends avoiding it during pregnancy. The good news: melasma frequently resolves after delivery, and safer alternatives exist in the meantime.
High-dose salicylic acid (BHA) Low-concentration, rinse-off salicylic acid (as in a face wash) is generally considered low-risk. However, high-dose leave-on products — 2% BHA toners, spot treatments, exfoliating pads, and chemical peel pads — are typically avoided during pregnancy due to greater absorption potential. Oral salicylates are not safe in pregnancy, which informs the caution around concentrated topical forms.
Chemical sunscreen filters: oxybenzone and octinoxate These chemical UV filters are absorbed through the skin and have demonstrated endocrine-disrupting activity in laboratory studies. While conclusive human harm data is limited, many dermatologists recommend switching to a mineral sunscreen (zinc oxide or titanium dioxide) during pregnancy as a precautionary measure. Mineral sunscreens sit on top of the skin rather than being absorbed and are considered safe throughout pregnancy.
Other ingredients to avoid: Formaldehyde-releasing preservatives (found in some nail polishes and hair treatments), high-dose phthalates, and isotretinoin (oral Accutane — a hard stop during pregnancy with documented teratogenicity).
Ingredients That Are Safe to Use
Mineral sunscreen (zinc oxide, titanium dioxide): Not only safe — essential. Sun protection during pregnancy is especially important because hormonal changes make the skin significantly more susceptible to hyperpigmentation and melasma. Daily SPF 30 or higher is the single most effective thing you can do for pregnancy-related skin changes. A broad-spectrum mineral sunscreen protects against both UVA (aging and pigmentation) and UVB (burning) rays without systemic absorption concerns.
Vitamin C (ascorbic acid): A safe and effective brightener and antioxidant during pregnancy. Vitamin C inhibits melanin production through a different pathway than hydroquinone, making it an appropriate alternative for managing hyperpigmentation and uneven tone. It also supports collagen synthesis — relevant for skin elasticity as the belly grows.
Niacinamide (Vitamin B3): One of the most versatile pregnancy-safe ingredients available. Niacinamide reduces inflammation, minimizes pores, improves skin barrier function, hydrates, and has clinically demonstrated efficacy for fading hyperpigmentation. It works well alongside vitamin C and is well-tolerated by sensitive skin — which pregnancy often produces.
Azelaic acid: A naturally occurring acid with anti-inflammatory, antibacterial, and skin-brightening properties. It is considered safe during pregnancy and is particularly useful for treating both acne and hyperpigmentation — two of the most common pregnancy skin concerns. It is available over the counter at lower concentrations (10%) and by prescription at higher concentrations (15–20%).
Hyaluronic acid: A deeply hydrating humectant that draws moisture into the skin and supports the skin barrier. Completely safe during pregnancy and excellent for managing the dryness and sensitivity that many women experience, especially in the third trimester.
Glycolic acid (low concentrations): A gentle alpha hydroxy acid (AHA) that exfoliates and improves skin texture. At lower concentrations (under 10%) and in rinse-off formulations, glycolic acid is generally considered safe in pregnancy and is frequently recommended as a retinol alternative for addressing texture and fine lines. Avoid high-concentration glycolic peels.
Benzoyl peroxide (low concentrations): Only about 5% is absorbed systemically, and it is metabolized before reaching the bloodstream. Most dermatologists consider low-concentration benzoyl peroxide (2.5–5%) safe for treating pregnancy acne. Avoid high-strength formulations and limit application to affected areas.
Topical clindamycin and erythromycin (prescription): Both antibiotic topicals are considered safe in pregnancy and are commonly prescribed for pregnancy-related acne when other measures are insufficient.
Managing Common Pregnancy Skin Concerns
Melasma (Mask of Pregnancy) Melasma appears as darkened patches on the forehead, cheeks, upper lip, and jawline — triggered by estrogen-driven increases in melanin production. It affects a significant proportion of pregnant women and is more pronounced in women with darker baseline skin tones. The most important intervention is diligent, daily sun protection — UV exposure worsens melasma significantly. Safe topical approaches include vitamin C, niacinamide, and azelaic acid. Most melasma fades postpartum, particularly with consistent sun protection after delivery.
Pregnancy Acne Surging progesterone increases sebum production, which can trigger or worsen acne — particularly in the first trimester. Safe options include gentle non-comedogenic cleansers, low-concentration benzoyl peroxide, azelaic acid, niacinamide, and topical clindamycin (by prescription). Avoid retinoids and high-dose salicylic acid. If acne is severe, a dermatology referral during pregnancy is appropriate.
Stretch Marks Stretch marks (striae gravidarum) develop as the skin stretches rapidly and collagen fibers in the dermis are disrupted. They are extremely common — affecting the majority of pregnant women — and are influenced significantly by genetics, not just skin care. While no topical treatment has been definitively proven to prevent stretch marks, consistent moisturization supports skin elasticity and hydration. Safe options include cocoa butter, shea butter, hyaluronic acid serums, and plant-based oils (rosehip, sweet almond, jojoba). Apply to the abdomen, breasts, hips, and thighs starting in the second trimester.
Sensitive or Reactive Skin Pregnancy hormones frequently alter skin sensitivity — products tolerated before pregnancy may suddenly cause irritation or flushing. Simplify your routine: a gentle fragrance-free cleanser, a barrier-supportive moisturizer (look for ceramides, hyaluronic acid, or glycerin), and daily mineral sunscreen is a complete and safe pregnancy skincare routine. Fragrance — synthetic or natural — is one of the most common triggers of skin irritation in pregnancy and is worth eliminating from your routine during this period.
A Quick Reference Guide
| Ingredient | Status | Notes |
|---|---|---|
| Retinol / Retinoids | ❌ AVOID | All forms — OTC and prescription |
| Hydroquinone | ❌ AVOID | High systemic absorption |
| Chemical sunscreens (oxybenzone) | ❌ AVOID | Switch to mineral SPF |
| High-dose salicylic acid (>2% leave-on) | ⚠️ LIMIT | Low-concentration rinse-off generally fine |
| Mineral sunscreen (zinc oxide) | ✅ SAFE | Daily use strongly recommended |
| Vitamin C | ✅ SAFE | Brightening, antioxidant, collagen support |
| Niacinamide | ✅ SAFE | Brightening, barrier repair, anti-inflammatory |
| Azelaic acid | ✅ SAFE | Acne and hyperpigmentation — safe in pregnancy |
| Hyaluronic acid | ✅ SAFE | Hydration and barrier support |
| Glycolic acid (low concentration) | ✅ SAFE | Gentle exfoliation; avoid high-dose peels |
| Benzoyl peroxide (low concentration) | ✅ SAFE | Limit to affected areas |
| Cocoa butter / shea butter / plant oils | ✅ SAFE | Stretch mark prevention and moisturization |
Always read full ingredient lists, not just product marketing claims. When in doubt about a specific product or ingredient, your OB, midwife, or a board-certified dermatologist is the right resource.
The Bottom Line
A healthy pregnancy is built on a foundation of consistent prenatal care, quality nutrition anchored by folate, iron, DHA, and whole foods, appropriate physical activity, adequate hydration, attention to mental health, and the knowledge to recognize when something requires urgent attention.
It is also built on awareness — of the care you deserve, of the disparities that exist, and of the fact that you are allowed to ask more of the system than it has historically offered.
You deserve care that is thorough, respectful, and responsive to your whole picture. If the guidance in this post helps you walk into your next prenatal appointment with more clarity or more confidence — that is exactly the point.
For related reading, explore our posts on prenatal vitamins and what the evidence supports, understanding your menstrual cycle as a health indicator, how social connection affects your health, how to maintain a healthy weight, and smart ways to fight acne.
References:
- CDC. Maternal Mortality Rates in the United States, 2024. NCHS Health E-Stats. March 2026.
- March of Dimes. CDC Issues New Data on Maternal Mortality Rates in the U.S. March 2026.
- ACOG. Tailored Prenatal Care Delivery for Pregnant Individuals. April 2025.
- ACOG. New ACOG Guidance Recommends Transformation to U.S. Prenatal Care Delivery. April 17, 2025.
- Safarzadeh A. Dismantling inequities to end the Black maternal mortality crisis in the United States. Int J Equity Health. 2025;24:114.
- Kamijo et al. Racial Disparities in Maternal Mortality Before, During, and After the COVID-19 Pandemic. PMC. 2025.
- ACOG. Nutrition During Pregnancy FAQ.
- ACOG. Exercise During Pregnancy FAQ.
- NIH Office of Dietary Supplements. Iron Health Professional Fact Sheet.
- National Academies of Sciences. Weight Gain During Pregnancy: Reexamining the Guidelines. 2009.
- FDA. Advice About Eating Fish During Pregnancy.
- CDC. Hear Her Campaign — Urgent Warning Signs During Pregnancy.
- Postpartum Support International. Helpline and Resources.
- National Academies of Sciences. Dietary Reference Intakes for Water. 2004.
- American Academy of Dermatology. Dermatologist-Approved Pregnancy Skin Care.
- Chua-Gocheco A et al. Safety of skin care products during pregnancy. Can Fam Physician. 2008. PMC3114665.
- Yaghi M, Baboun D, Keri J. Acne and Pregnancy: A Clinical Review and Practice Pearls. Cutis. 2024;113.
Bottom Line: Healthy Pregnancy
Before you’ll be able to take care of your little munchkin, it’s important to take care of yourself first. Your unborn baby is just waiting to slurp up all those nutrient-rich foods from all the food groups such as whole grains, fruits and vegetables, proteins and healthy fats. Keep your healthcare provider posted of your dietary choices and let him/her provide you a personalized health guide with additional supplements if needed.
Sign up to NubianDoc and stay updated with the latest health information.